










HYBRID BONE MARROW ASPIRATE, THE BEST OF BOTH WORLDS!
There is a continuing debate between using bone marrow aspirate in a non-centrifuged manner and using it in a manner where it is concentrated by centrifugation. Until recently bone marrow aspirate was essentially always concentrated. This question has generated much discussion and some heated debates in the Regenerative Medicine circles. The question is which group is correct? My answer is that both groups have valid points why their technology is the correct path to take. For this reason, we have come to the conclusion that a hybrid utilizing both centrifuged and non-centrifuged marrow aspirate works best. Bone marrow aspiration is very much technique driven regardless of the final preparation method. The purpose of this blog is not to discuss techniques but rather discuss aspects of centrifuged, non-centrifuged, and a hybrid marrow aspirate.
For some time now, we have been performing what we call the Purbred-HybridTM technique. We are utilizing both centrifugation and non-centrifugation to prepare our marrow. We realized that both preparation methods have their benefits. It has seemed to make a difference in our results clinically. Some time ago I became aware that centrifuging bone marrow may also have some drawbacks. We started doing some research on this subject. One question we started to ask is if there are some cells that are being discarded by centrifugation?
We felt that one type of cell that was being discarded was a V-Cell. This is a very unique stem cell. It is actually called a Very Small Embryonic-Like Stem Cell. In characteristics, it is very similar to an early CD-133 stem cell. There is still some controversy concerning V-Cells. I have previously written about this cell and do not wish to belabor the issue in this blog. We feel that V cells definitely have a contribution. This may be one of the more controversial differences between the two bone marrow preparation methods since V cells are not universally accepted. However, I would like to move past V cells instead keying in on other significant differences.
The biggest discussion points for those favoring centrifugation is that centrifugation will result in a concentration of stem cells from the bone marrow aspirate. Those people in favor of centrifugation feel that taking a larger amount of marrow aspirate and then centrifuging it will give more stem cells. Typically, the type of stem cell we are talking about is a mesenchymal stem cell (MSCs). There is little dispute to this fact. I agree with it one hundred percent. The real question to ask are the mesenchymal stem cells the most important regenerative cell to enable success? There is no clear-cut answer to this question. However, we are becoming increasingly aware that a symphony of cells is needed for success. We need to move beyond the juvenile thoughts that the MSCs are really the only important cells in marrow aspirate. MSC numbers may be an indication of good aspiration techniques but does this translate into good clinical success? Are we cutting our nose off to spite our face? In our quest to increase MSC numbers by centrifugation are we sacrificing critical components of the marrow aspirate? Let us take a look at both sides of the issue.
What are some of the other benefits of centrifugation? Centrifuging does have benefit by stressing the cells. It can turn on certain metabolic switches driving the cells to repair and may well cause the production of a greater volume of growth factors. When all is said and done growth factors are important contributors to success in regenerative procedures. The growth factors work in many different directions including reducing local inflammation and at the same time encouraging repair. Centrifugation also has a positive effect on MUSE BM stem cells. Muse cells are pluripotent and can endure stressful situations such as those found in the joint. The stress of centrifugation may actually help the Muse cell since they by and large thrive in stressful situations. But not all is good since centrifugation probably will eliminate some of the Muse cells from the final product. Another negative side of centrifugation, is the fact that it will change the shape of many cells and the number of cilia and thus the cell surface receptors. Therefore, I believe, it will inevitably change the performance of the stem cells and other regenerative cells. So, we can see there is no clear-cut advantages of either technique.
Let us look at other advantages we get with centrifugation and non-centrifugation. Right off the bat we need to look at megakaryocytes and platelets. These cell types are what gives differentiation issues in bone marrow aspirate versus bone marrow concentrate. The bone marrow aspirate will contain more platelets so it will cause a different profile of cytokines. The cytokines from the platelets will cause the differentiation of cells to take on a different path, mainly hematopoietic differentiation. We know hematopoietic stem cells are one of the main drivers of tissue regeneration (the mesenchymal stem cell is important for immune modulation). For years we have been adding an additional PRP with every bone marrow injection. This seems to be a good equalizer.
Platelets may be a small difference between centrifuged and non-centrifuged marrow aspirate. The platelets are easy to add thus the difference can be equalized. There are some other components that are not so easy to add and they are lost in some of the centrifugation processes. One of these components is exosomes. The following diagram gives us an idea about exosomes. Exosomes are much like the body’s Fed-Ex system. They deliver growth factors where they are needed. The exosomes contained in virgin aspirate may be more potent and more numerous
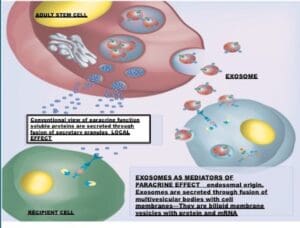
than those found in centrifuged marrow. Many times, when we wish to concentrate exosomes we will use ultra-centrifugation. We are not sure of the overall effect that centrifugation has on exosomes but chances are we will lose some exosomes to centrifugation and possibility change their secretory profile. We must also realize exosomes maybe a product of the cell environment. The various cells can sense what type of growth factors may be needed based on their environmental stimuli. Centrifugation may affect the stimuli.
The neutrophils also play a huge role here in the two versions of bone marrow. The neutrophils basically control the oxygen uptake or “respiratory burst” that is so important to the viability of stem cells, especially vascular stromal cells. The respiratory burst does both good and bad. A respiratory burst will release free radicals (ROS) which can be bad for the overall environment of the regenerative cells (however they are very good at killing pathogens). At the same time the ROSs can have a profound effect on intracellular signaling pathways and ultimately in modulating gene expression. This following diagram shows the paradoxical effect of levels high free radicals on cells:
The opposite effect occurs in low levels of ROS.
Recent data have revealed that the respiratory burst is closely related to inflammation resolution in many instances. What else does the respiratory burst accomplish? Neutrophil respiratory burst-induced hypoxia activates macrophage erythropoietin signaling to promote acute inflammation resolution. This signaling is activated following inflammation. Pharmacological or genetic inhibition of the respiratory burst suppresses hypoxia and macrophage erythropoietin signaling. An interesting experiment was performed. In this experiment, a Macrophage-specific erythropoietin receptor-deficient mouse having chronic granulomatous disease (CGD) was utilized. These mice lacked the capacity for a respiratory burst, displayed impaired inflammation resolution and had symptoms of GCD. When given exogenous erythropoietin it enhanced this resolution of the CGD.
How does centrifugation come into play here? Mechanical stress like centrifugation causes major changes through reduced oxygen uptake especially in neutrophils. Centrifugation can negatively affect the “respiratory burst”. The reduced uptake of oxygen by the neutrophils caused by the mechanical stress of centrifugation will have a profound effect on transduction and differentiation and thus on the success of the bone marrow graft. There will be observable differences in the number of different cell types as well as in the downregulated pathways such as Macrophage 1 and Macrophage 2 conversion.
Macrophages have developed a unique ability to radically change their metabolism from a heal/growth promoting function, now known as M-2, to an inhibit/kill function, now known as M-1. This conversion is many times dependent on the “neighborhood” the macrophage is found. This neighborhood is the extracellular matrix. The macrophages are the center of the immune “solar system”. Through these innate responses, macrophages are the central controlling element for tissue integrity and host defense while at the same time directing other cells of the immune system. The following diagram is a good example of this concept.
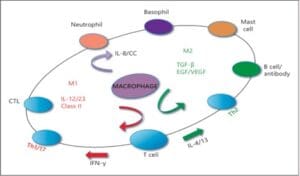
We must ask the question which of these cells are we discarding with centrifugation. We must remember innate immune cells such as basophils and mast cells and other adaptive cells produce IL-4 and IL-13 priming M2 macrophage. IL-4 induced M2 macrophages expressed high concentration of IL-10, IL-1R antagonist, chemokines CCL22 and CCL17, and intracellular enzyme arginase-1. All of these ensure the recruitment and activation of immune response and immune-suppressive function of M2 macrophages. In addition to immune response, IL-4 induced macrophages stimulate arginase activity by converting arginine to polyamines and collagen precursors that are crucial for tissue modeling and wound healing. Macrophages were shown to be responsible for regeneration by actively metabolizing arginine with arginase into ornithine and urea. This is of upmost importance since macrophage production of ornithine is required for many repair processes because it is a precursor of the polyamines required for cell proliferation and collagen synthesis for extracellular matrix construction.
The M-1/ M-2 conversion is of extreme importance. We now know that M-1/ M-2 macrophage conversion can have a significant bearing on the ultimate success of a bone marrow graft. The following diagrams show this concept:
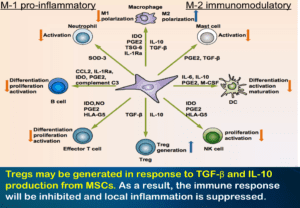
These slides show the relationship between the stem cells and the different types of macrophages. The environment that the macrophages are found determines what pathway they ultimately go down. Macrophages in M1 inhibit mode direct T cells to pro- duce Th1-like cytokines (e.g. IFN-γ) that stimulate specific cytolytic T cells and activate more M1 macrophages. In contrast, macrophages in the M2/ heal mode stimulate T cells to produce Th2-like cytokines (e.g. IL-4 and TGF-β) that cause B cell proliferation and antibody production and further amplify M2 responses such as collagen precursors. Thus, macrophages actually use T cells as the ‘middle man’ to further amplify M1 or M2 dominant responses. In this case the various cells of the immune system may be adversely affected by centrifugation. This can interfere with the M-1/M-2 conversion axis pushing it more towards the M-1 (inflammation) and away from M-2 (repair). This can have a profound effect on success of a bone marrow aspirate.
We can see that a bone marrow aspirate is much more than just mesenchymal stem cells. It involves a symphony of cells from the immune system. We are now very much aware that MSCs alone are not the only immune modulator nor are they the only mediators cell repair. The cells of the immune system are very much involved in the success or failure of a regenerative medicine procedure. We need to realize that many different cells such as MSCs, HSCs, and the whole array of immune cells are important for regenerative success. Our techniques for marrow aspiration have improved and at the same time so has our final product. I have gone from full centrifugation to no centrifugation to now the hybrid combining both techniques.
To quote one of my favorite Beatles songs “It’s been a Long and Winding Road” to come to these conclusions. We can now see that both centrifugation and non-centrifugation both have their merits and their drawbacks. We became aware of this some time ago and have used a hybrid technique (centrifuged and non-centrifuged marrow) for some time now. Our results are clinically better. In our final hybrid product, the unspun marrow aspirate predominates in volume over the centrifuged marrow aspirate. However, more marrow aspirate is harvested for centrifugation than non-centrifugation. I am also fortunate that in some of my clinics I have the ability to utilize a variety of cytokines such as IL-4 which helps regeneration by influencing macrophage polarization. As time goes on I am sure more changes to the hybrid protocol will be made. One thing I am sure about is that this is an ever-changing field that always requires rethinking and reevaluation.
Thanks,
– Dr. P
